By Mark Giammalvo
|
By Mark Giammalvo |
|
|
What would you think if you saw this sign posted in the window of a business? It would get your attention and maybe even a few laughs. Unfortunately, the topic of health care is no laughing matter. Health
care benefits are becoming increasingly important in the struggle to keep
good employees. Are you aware of all your options? It seems like things were
so much simpler just a few years ago. Regarding health care, at one time
most businesses had the same insurance company. You remember: the old 80/20
indemnity plans with the quarterly deductible? The patient paid 20 percent
of the office visit plus the quarterly deductible, and the insurance provider
paid the remaining 80 percent. I don't know if it was good or bad, but it
sure seemed a lot simpler. A major chore
In addition, we enlist the help of a broker who obtains quotes form several different companies each year. Even so, every year I am shocked over our renewal rates. In the past, they have gone from chunky 12 percent to whopping 30 percent increases. These increases are tough to stomach for both the employer and the employees. Currently we pay 50 percent of our employee's health care benefit. Even so, how do you tell your employees every year that their weekly pay just took another $20 hit? How will the business cover a $5,200 annual increase? Let me tell you, it's just not easy. In the end, it comes down to several key issues. At
first blush, the health care market can seem like a labyrinth of nightmares.
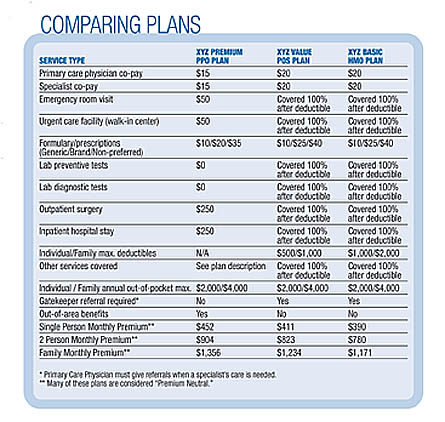
There are many companies to choose from and each company has a variety of
plans and configurations. One company will offer a two-tier rate as Single
vs. Family coverages. Other companies will offer three- or four-tier plans
that include the two-person households (Single Plus One). Once you know the
rate, the business and employees can figure their annual costs. That's the
easy part. The hard part is choosing a plan everyone can best live with. What's your style? Will your family have to go to the hospital this year? If so, can you handle the first $2,000 out-of-pocket expenses? Do you and/or your employees require many maintenance prescriptions on a regular basis? Can you handle a formulary (drug) benefit of 10/25/40? It's a lot to think about. Don't be surprised if the insurance company makes you fill out a questionnaire concerning details of how you pay your insurance. A common question on this form is what percentage your business pays toward employee health care. Typically the insurance companies will mandate that the business pay at least half of the family plan's premiums and a third or more of the single plan's premiums. Why would the insurance company care what portion your business pays? It all has to do with the insurance underwriters and how they determine risk ratios. A business that pays for half of the health care benefit will tend to have a better ratio of healthy subscribers. The logic is that more people will sign up because a larger amount is employer paid, and that means more healthy people in the plan. But when the employee has to pay more, those who know they are more likely to need health care coverage will tend to sign up more readily. This is because they have no choice but to purchase the coverage. This ends up costing the insurance company more money. Other questions on the questionnaire may ask about
the number of "eligible" employees that are currently not on the plan. This
normally means other full-time employees who are obtaining health care elsewhere,
such as through their spouse's employment. Again, the insurance company wants
to know about possible future risk. The insurance company knows that they
may be on the hook for providing coverage if an employee's spouse suddenly
loses his or her job or heath care. Unanticipated increases However,
the insurance company decided to slip in an additional rate this year. Even
my health care broker had never heard of it. After choosing our renewal plan
we were stunned when we received our first bill. When I called the representative at the insurance company, he directed me back to my rate quote sheet. Sure enough, down at the bottom, was a statement that said that we had two "Medicare Active Employees." On a subsequent conference call, my insurance broker and I challenged the account representative over this new unannounced rate structure. The account representative had a few interesting explanations. He said that in the past, overall group rates were higher to make up for the "older high-risk" members on Medicare. The insurance company had decided to spread out the risk factor in a more realistic way. Another words, give more premium burden to the Medicare-active members. However, federal law dictates that Medicare is the primary provider when a Medicare active participant is on a plan with 20 members or less. That being said, why would the insurance company charge more if Medicare were the primary responsible provider? The representative's answer was interesting: He said that a person who is on Medicare and still on a private plan is considered a "red flag" with the underwriters. Why? Because underwriting presumes that member must have a high-risk health factor if they need both the Medicare and a private plan. Needless
to say, we did not get very far in the discussion. Our broker believes that
they quietly pushed this new three-tier structure through in hopes of catching
most subscribers off-guard. It would have been nice for them to bring this
change to our attention before we chose the renewal plan. Then we would have
had a truer picture of the coming year's cost. Don't forget details In
addition, the insurance companies can offer incentives to doctors that stay
within the pool amount for the year. Doctors that overutilize care with too
many specialists referrals may not receive the dividend payment. Some patients
and physicians argue that this method reduces the utilization of services
and even compromises patient care. Others counter that the plan is fair and
unbiased. Buyer beware If
you belong to an association, check on whether health care is offered through
that organization. If you are not an automotive association member, visit
the Internet site of the U.S. Small Business Administration (SBA) at
www.sba.gov.
Search for AHP or Association Health Plans. These plans have been proposed
in Congress to allow groups of small businesses to band together to buy health
insurance. According to SBA, some of the projections are that businesses
could save as much as 13 percent on their coverage by taking advantage of
AHPs. The U.S. House of Representatives passed the legislation in 2003, and
the Senate is due to take up the matter next. Arm yourself with data

|